Hysteroscopy
Introduction
Hysterectomy involves surgical removal of the womb or the uterus. This surgery is commonly performed due uterine fibroids or benign tumors of the uterus, abnormal bleeding from the uterus, endometriosis or cancer.
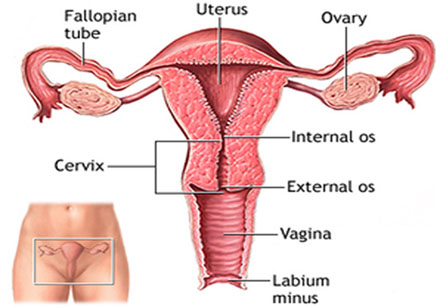
A total hysterectomy involves removal of the uterus, both the fallopian tubes, both ovaries and the cervix. A radical hysterectomy involves removal of the uterus, cervix, and part of the vagina, tubes, ovaries and sometimes tissues surrounding the uterus. This type of hysterectomy is performed in cervical cancers.
Most women recover from this operation with no complications. But as with other major surgeries, hysterectomy is associated with the risks of pain, bleeding, infections, nerve or urinary bladder or bowel injury and anesthetic complications like heart attack and stroke.
Hysteroscopy is a procedure that allows your doctor to look inside your uterus in order to diagnose and treat causes of abnormal bleeding
Non surgical alternatives to hysterectomy include medications and hormonal therapy. A surgical alternative is removal of the tumor alone. Once these fail a hysterectomy needs to be considered. Uterine artery embolization is a newer alternative.
Before the surgery is undertaken a general health checkup is mandatory. You will also need to undergo a complete pelvic examination, a pelvic ultrasound examination and a pap smear. These tests will help your gynecologist decide on the severity of your disease and also the type of hysterectomy that you may need.
Procedure:
You will need to be empty stomach for 6 to 8 hours before the surgery. Usually a light dinner is recommended. Food or water in the stomach when under anesthesia can go into your lungs and may even cause death. The hairs in your pubic region will be shaved off or removed with hair removing cream on the day before the operation. Once inside the operation theatre an intravenous line will be made in one of the veins of your fore arm. You may be given medications to allay anxiety before the operation. Instruments to monitor your heart rate, rhythm (using EKG), blood pressure and oxygen saturation (to detect adequacy of breathing) will then be plugged in. A urinary catheter is placed to drain off the urine during and after the operation. Usually general anesthesia or regional anesthesia is advocated for hysterectomy. With general anesthesia you will be made unconscious during the operation with a breathing tube – endotracheal tube in place to help you breathe through a breathing machine or ventilator. If the operation is performed under regional anesthesia for example spinal, epidural or caudal anesthesia, an anesthetic injection in your spine will make you numb waist down during the operation. With regional anesthesia you will remain conscious and comfortably sedated during the operation.
Two common approaches to hysterectomy are the abdominal and vaginal. As the names suggest abdominal hysterectomy is performed via a surgical incision over the abdomen and vaginal hysterectomy is performed through the vaginal wall.
In an abdominal hysterectomy, your abdomen will be cleaned with an antiseptic solution. Thereafter sterile surgical drapes will be placed over it. A 6 to 8 inch incision will be made either vertically from your navel to pubic bone or horizontally running along the top of the pubic hairline. Once the uterus and its surrounding structures are exposed, all the major blood vessels are tied up and the uterus along with the tubes, ovaries and cervix is removed by dissection. The cut end of the vagina from where the cervix has been removed is tied up. The vagina is checked for bleeding. After the surgery is completed skin is sutured or stapled leaving a drainage tube in place to drain out the excess fluids. The operative site is then bandaged.
After the operation you will be taken to the recovery area where you will be awakened and given medications for pain relief.
In a vaginal hysterectomy the skin around the vagina is swabbed with antiseptic lotion and sterile drapes are placed over it. Your legs will be spread and raised comfortably to be placed in stirrups to facilitate the operation. A speculum is used to hold the vagina open for better visualization of the operative field. The surgeon will make a circular incision around the cervix in the upper part of the vagina. The tissues in and around the uterus will be exposed and similar to abdominal hysterectomy the major blood vessels will be identified and tied off. The uterus, tubes, ovaries and the cervix will then be dissected out of the vaginal incision. The vaginal incision is then sutured off leaving a drainage tube to drain off the excess fluids. The vaginal opening will then be packed in sterile gauze and closed.
After the operation you will be taken to the recovery area where you will be awakened and given medications for pain relief. After your vital signs are stabilized you may be shifted to the hospital bed. In most cases you may need to stay for up to a week in the hospital. You will be given antibiotics and pain relievers for a few days after the operation. You will need around 4 to 6 weeks to recover fully. Recovery is more rapid with vaginal hysterectomy. Abdominal hysterectomy is also associated with higher rates of pain and infections compared to vaginal hysterectomy.
Do not lift weights or exercise for a few weeks after the operation. Any bleeding, fever or increase in pain needs to be brought to the attention of your caregiver immediately. You can indulge in sexual intercourse only 6 weeks after the operation or later if your doctor so advises. If you have not reached menopause at the time of the operation, this operation might bring menopause and the adverse effects associated with menopause due to removal ovaries. Thus you can experience weight gain, hot flushes and dryness of vagina after hysterectomy.